ASC Billing Services for
Ambulatory Surgical Centers
Getting paid for surgical care has never been more complex. OmniMD makes it simple, precise, and consistently above 97%.
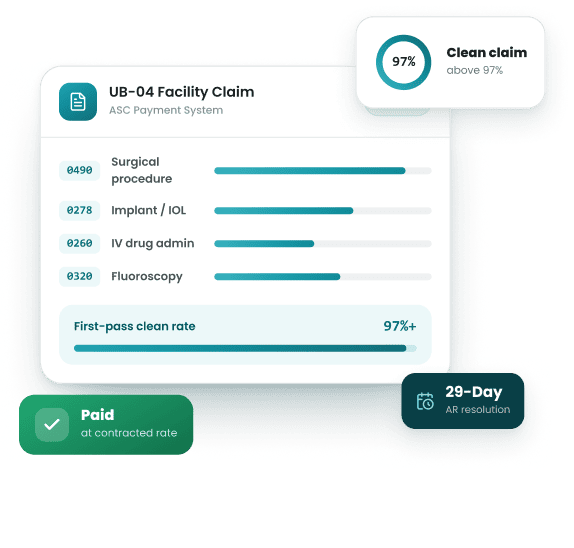
97+
Clean claim rate
29-Day
AR resolution
ASC
Credentialed coders
HIPAA
Compliant
The Structural Difference That
Makes ASC Billing a Category of Its Own

ASC Facility Fee Billing vs. Physician Billing
Every surgical case generates two independent claims under two entirely different systems. The surgeon files on CMS-1500. The ASC files on UB-04. General billing companies know one. OmniMD manages both under a single operation, eliminating the revenue gap that forms when facility billing and physician billing are handled separately.
This includes


UB-04 revenue code map
auto-assigned
0490
Primary surgical procedure line
0278
Implants, joint hardware, IOLs, bone grafts
only pays separately above CMS device-intensive threshold
0300
IV drug administration
must pair with a separately payable drug code
0490
Primary surgical procedure line
0320
Fluoroscopy guidance
requires correct imaging guidance code pairing
ASC Revenue Codes and UB-04 Claims
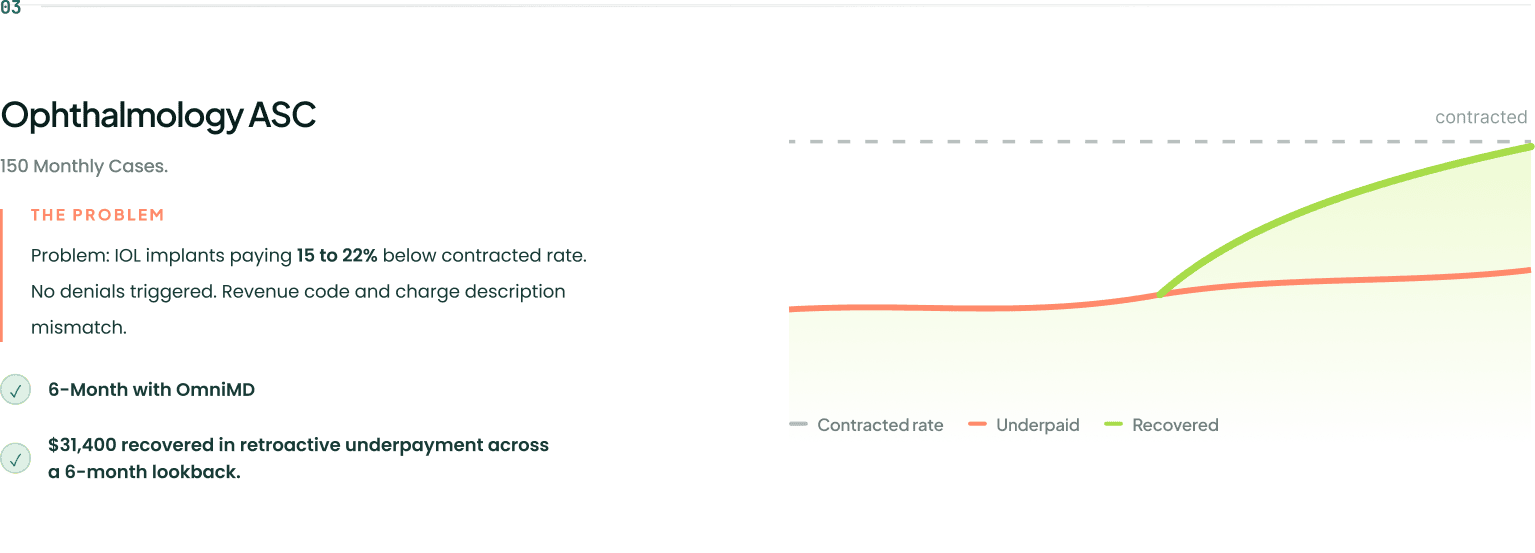
Wrong revenue codes rarely produce denials. They produce payments 15–22% below contracted rate, silently, with no alert from the payer.
OmniMD automates correct code assignment and adds
human review on all high-dollar cases, covering:
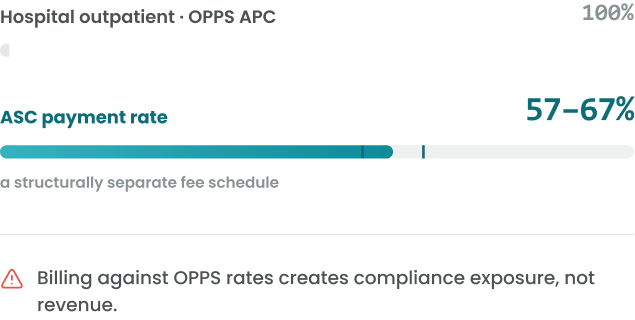
Medicare ASC Billing Rules
ASC payment rate is 57 to 67% of OPPS APC : a structurally separate fee schedule. Billing against OPPS rates creates compliance exposure, not revenue.
We ensure correct application of:
How OmniMD Manages Every Stage
of Your ASC Revenue Cycle

ASC Charge Capture and Billing and Coding
We deploy ASC-credentialed coders who work exclusively on surgical center
cases, driving accuracy at the point of charge entry.
This includes
ASC Facility Claim Submission (UB-04)
We construct every UB-04 with the precision a payer audit demands, transmitting to 50+ payers with payer-specific rules pre-applied.
This includes

ASC Revenue Cycle Management
We manage the full revenue cycle from 48 hours before the patient arrives
through final collections, improving speed, accuracy, and yield across:


Denial Management for ASC Claims
We trace denials to their origin, not just their outcome. Resubmission without root
cause analysis means the same denial returns next month.
Our process drives results through


ASC Billing Compliance and Audits
The OIG flags ASC billing annually for implant charges, high-risk procedures, and
modifier accuracy. We stay ahead of it.
This covers

ASCQRP Billing Support
We protect your full Medicare ASC payment rate by managing ASCQRP
obligations year-round:
This covers
ASC Billing Services by Specialty

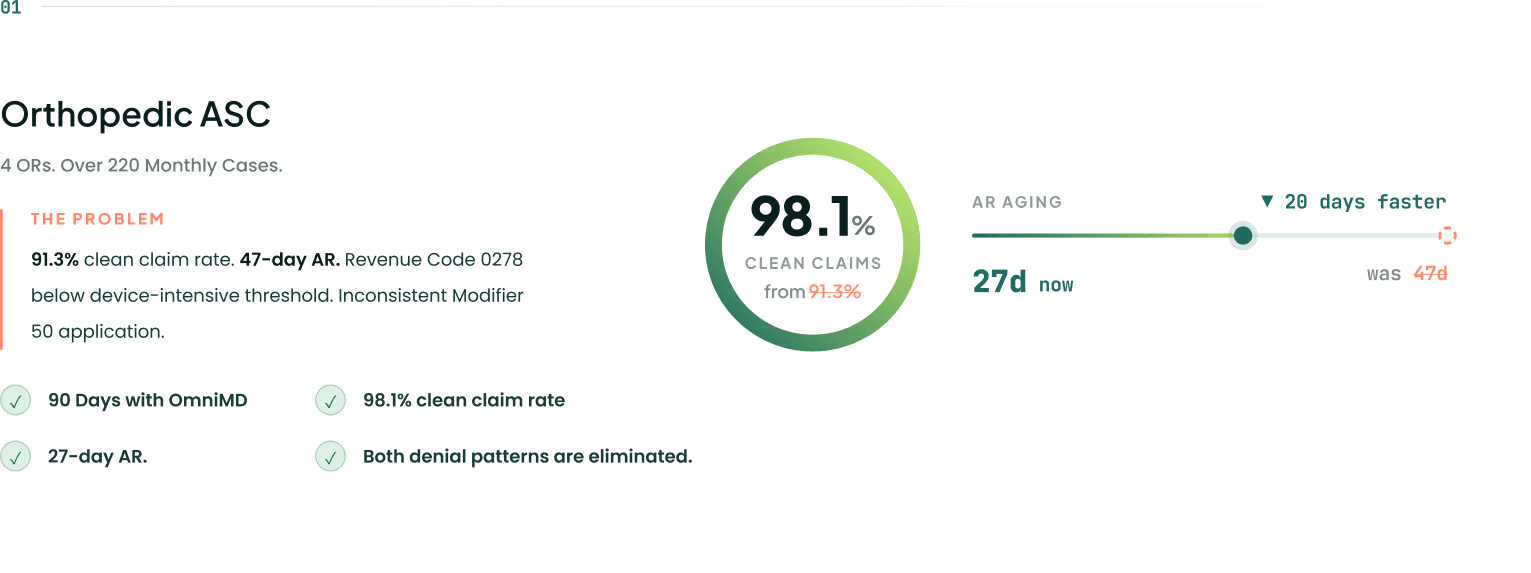
Orthopedic ASC Billing
Highest dollar-per-case complexity in ambulatory care. We manage the billing risks that cost orthopedic ASCs the most:


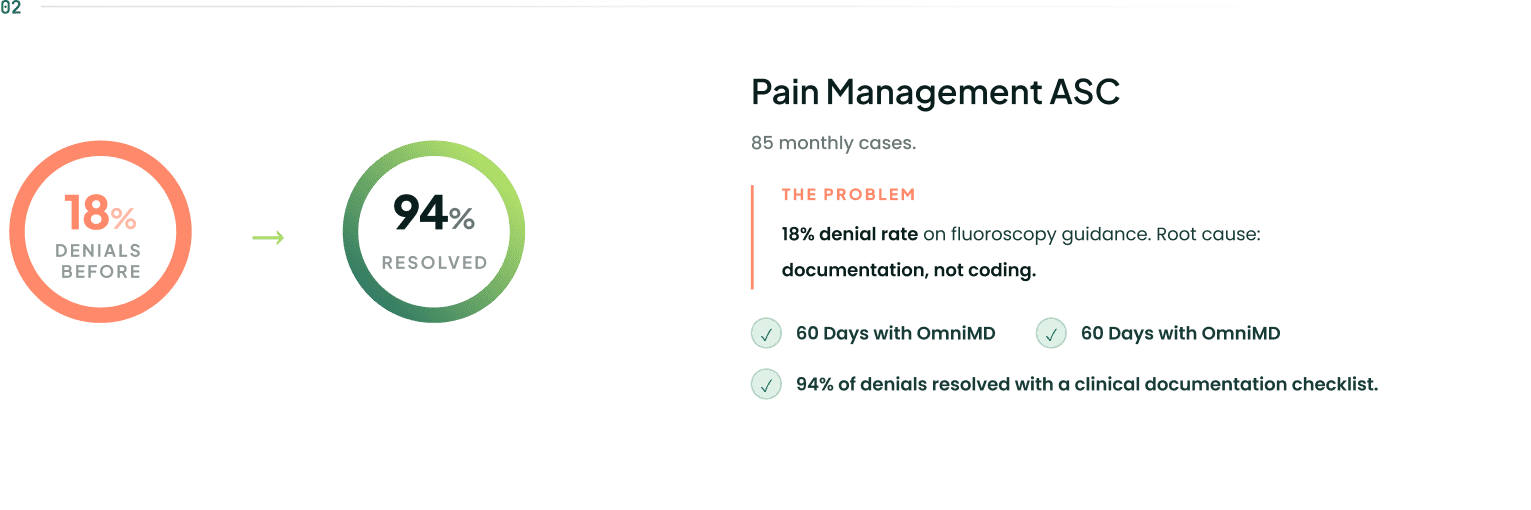
Pain Management ASC Billing
Fluoroscopy guidance denials in this specialty are almost always documentation failures, not coding errors. We prevent them through:

Ophthalmology ASC Billing
Bilateral cataract rules differ by session type. Wrong application produces a payer dispute and a patient billing complaint at the same time. We manage it through:

GI and Endoscopy ASC Billing
The screening-to-diagnostic conversion is the most complaint-generating billing event in this specialty. We manage it through :

| Capability | General Billing | Hospital RCM | Enterprise RCM | OmniMD |
|---|---|---|---|---|
| ASC facility fee expertise | Rarely | — | Frameworks only | Operational daily |
| UB-04 and ASC revenue codes | Limited | Sometimes | Not in scope | |
| ASC-credentialed coders | — | — | — | |
| ASCQRP support | — | — | — | |
| Implant billing at device threshold | Rarely | — | — | |
| ASC-specific denial root cause | — | — | — | |
| Clean claim rate | 85 to 90% | 88 to 92% | Varies | 97%+ |
What We Are Building with
Our ASC Billing Clients
Get your free ASC Billing Audit
Most ASC administrators lack precise visibility into three things: clean claim rate by payer, denial rate by procedure, and revenue code accuracy against current CMS guidelines. The OmniMD audit surfaces all three.
