
How to reduce claim denials by 50% in 90 days
You probably didn’t open this blog randomly. Chances are, someone just walked into your office (or pinged you on Slack) asking why denials keep climbing, and you’ve got maybe ninety days to come back with a real answer. The number in your head, 10%, 14%, 18%, whatever it is, isn’t going to fix itself.
Most plans for reducing claim denials fail. The tactics in them are usually fine, but they assume a practice that doesn’t really exist: one with clean data, a biller who has time, providers who reply to emails, and payers that behave consistently. If your practice is missing any of those things, a generic plan won’t get you very far in 90 days.
What actually works depends on what kind of practice you’re running. We see four versions of this problem more than any others, and what’s worth doing first is different in each.
The four scenarios at a glance
| Practice type | Top denial reasons | Biggest lever | Realistic 90-day result |
| New clinic (under 2 years) | Credentialing gaps, eligibility errors | Payer enrollment audit | 60 to 70% reduction |
| Established practice (10+ years) | Same 5 reasons for years | Breaking workaround habits | 50% reduction |
| Urgent care | Eligibility, prior auth on imaging, E&M disputes | Front-desk automation | 45 to 55% reduction |
| Multi-specialty group | Different per specialty | Specialty-by-specialty fixes | 50% reduction |
The next four sections go into each scenario in more detail. Most real practices are a mix, often two of these at once, but one usually dominates. Pick the closest fit and read the 90-day plan with that in mind.
#1: The clinic that opened in the last two years
In a newer practice, what looks like a denial problem is usually just paperwork that nobody finished. Provider enrollment is the big one, and there’s almost always at least one gap somewhere. The patterns we see most often:
- A provider whose group enrollment is done but whose individual NPI never got linked to the group’s TIN.
- An effective date that starts a week after the provider actually started seeing patients.
- A payer where the credentialing application sat in the portal because nobody saw the email saying it was missing a document.
- A CAQH attestation that expired quietly and took enrollment down with several payers at once.
- Medicaid managed care plans that needed separate enrollment beyond the parent Medicaid contract.
The codes that flag all this are usually CO-B7 and PR-242, though depending on the payer and the clearinghouse it might show up as something else.
The other thing is the front desk. Whoever is there was probably trained at a previous practice, and a lot of what they learned doesn’t really translate to your payer mix. The habits we see go wrong most often:
- Verifying eligibility on the wrong subscriber ID for spouses and dependents.
- Only running eligibility on new patients because that was the rule at the last clinic.
- Pulling the deductible once at the start of the year and assuming it still applies in October.
The work in the first 30 days is honestly pretty boring. Pull every provider’s enrollment status with every payer, in writing, from the actual payer portals. Don’t take your credentialing company’s word that you’re all set, because they’re often wrong about that. When you find gaps, file retroactive effective date requests. Medicare gives you 30 days for that, most commercial payers give 60 to 90 if you ask in writing inside the window. Some of those requests will get denied even when you’re clearly in the right. That just happens, and you have to budget for it.
For the front desk, training isn’t really the answer. Just sit next to whoever is running eligibility for a couple of hours and watch what they actually do. It’s almost always two or three specific habits, not a gap in what they know.
Newer practices tend to see the biggest improvement, and not because the work is clever. It’s mostly that the starting numbers were inflated by stuff that was never really an operational issue, just paperwork. We’ve seen new practices cut denials by more than half in the first month alone.
#2: The practice that’s been running for a decade or more
If you’ve been around for ten or more years, your denial pattern is probably the same one it was three years ago. And three years before that. The same five or six reasons keep showing up, the same biller works them, and the money eventually comes in. The numbers are bad, but they’re stable, and that’s part of why nothing has changed.
What you’re really up against here isn’t a denial problem in the usual sense. It’s a workflow that’s been doing this for so long, it might as well be carved into the wall. The biller has usually been there longer than anyone except the founding provider. The way they handle denials, like resubmitting with the right modifier, pulling notes for an appeal, calling the rep at the payer they have a relationship with, is not a workaround to them. That is just how they do their job. They have been doing it that way for a decade, and the practice has run on their work.
So when you ask them to change, it sounds like criticism, even when you don’t really mean it that way. They are the reason your AR has not blown up. You sit them down and say something like “we need to stop appealing and start fixing the underlying issue,” and what they hear is “you have been doing this wrong this whole time.” They will nod, they will agree, and then the next denial that hits their queue, they will go right back to what they were doing before.
So the real question in this scenario is whether the practice owner, who is usually also the lead provider and has been working with this biller for years, is willing to have an uncomfortable conversation. If the answer is no, the plan below stalls. We’ve watched this happen plenty of times. A denial comes in during week three, the biller goes back to what they have always done, the provider does not push back, and a few weeks of progress just unwind in a single afternoon.
If the answer is yes, the helpful thing to know is that the biller usually wants the easier life that root-cause fixes would give them. They do not want to be the bottleneck. They just do not want to be told they have been one. The conversation that actually works sounds more like “let’s stop doing all this rework” than “let’s fix what you’ve been doing wrong.” That is not just a framing trick, by the way. It is also true.
#3: Urgent care
Urgent care is just its own thing. The volume swings all over, the patient mix changes through the day, and a lot of people walk in with whatever insurance situation they happen to be in that day. A paper letter from the marketplace. A phone screenshot of an old insurance card. A Medicaid number scribbled on a Post-it. None of that is what your eligibility system was built to handle, and your front desk has maybe 30 seconds to figure it out.
A few patterns show up almost every time we look at urgent care denials:
- Eligibility errors at the top, but usually not because the check got skipped. The check actually ran. It just came back ambiguous, like active coverage but a different subscriber ID, or coverage with a high deductible the patient swears they don’t have. The front desk didn’t know what to do with the result, so they took the patient’s word for it.
- Prior auth denials on imaging. It is almost always the same scene. The provider ordered the CT, the patient was already in the room, and the auth was never going to come through in twenty minutes. We cover this pattern in full in our guide to prior authorization in radiology billing. The imaging happened, and the claim got denied.
- E&M level disputes. The provider documented at the end of the shift, from memory, an hour after the visit, and the documentation does not quite carry the level they billed.
The thing that makes this scenario different from the others is time. Anything you change, whether it is at the front desk, in the provider workflow, or in billing, has to fit in the seconds that already exist. You can’t add twenty seconds to intake at a clinic where the room target is six minutes. It just isn’t going to happen.
So in urgent care, the answer is mostly automation rather than process. Real-time eligibility built right into the intake tablet. Prior auth workflows that fire automatically when someone orders imaging. EHR prompts that flag missing documentation before the chart closes. Automation isn’t a silver bullet, to be clear. It works fine for patients with a clean active card, and it breaks for anyone whose situation is weirder, which is honestly a real chunk of the urgent care population. But the alternative is asking the front desk to do more in less time, which doesn’t work at all.
When you read the 90-day plan below, run everything through this filter: if a fix costs intake seconds and isn’t automated, it isn’t going to survive a busy Saturday.
#4: The multi-specialty group
Most multi-specialty groups got that way because someone bought a handful of practices and put them all under one TIN. The billing setup, the front desk training, and the management style usually came from whichever practice was acquired first or got the biggest, and now those same systems are being run for specialties they were never built for. That’s the underlying issue. Each specialty is having a denial conversation that the central billing team is not really set up for:
- Ortho is dealing with medical necessity and modifier 25 and 59 issues, which means the central biller, who probably came up in primary care or one specific specialty, is appealing things the provider could have prevented at the chart.
- Behavioral health is fighting documentation and unit calculation, a different ruleset that nobody on the central team is fluent in.
- Surgery is losing money inside the global period because the central biller doesn’t always know which post-op visits should have been billed separately.
- Cardiology is stuck on prior auth for diagnostics, and the central auth team is sized for a primary care load.
The trap people fall into here is launching one big denial-reduction project across the whole group. It feels like an efficient move, and it really isn’t. Your attention ends up spread across specialties, the central biller can’t go deep on any one ruleset, and progress just creeps along everywhere.
What we’ve actually seen work is treating each specialty as its own project, running in parallel. Each one gets its own diagnosis, its own list of top reasons, and its own owner. The central billing team is there to support, not to drive.
The complication, of course, is staffing. The right owner for each specialty is usually the specialty lead, and that person is almost always a producing provider with full clinical hours and very little spare time. So a chunk of this scenario is figuring out who in each specialty is actually going to spend two or three hours a week on this. If nobody can, that specialty isn’t going to move, and you should be honest about that up front rather than pretending it’ll work out.
The 90-day plan that works for all four
The four scenarios share one spine. The differences live inside each phase. Let’s see how.
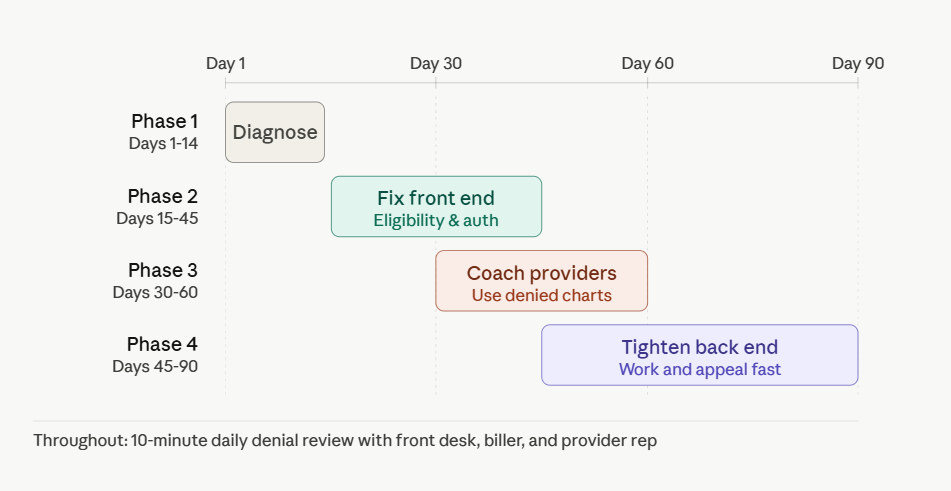
Days 1 to 14: Quantify before you fix
You’ve already got a working theory from the scenario above. What you don’t have yet is the dollar damage, the payer-by-payer breakdown, and the baseline you’ll measure progress against. That stuff comes from your own data.
Pull every denial from the last 90 days into a spreadsheet, then sort it three different ways: by CARC and RARC code, by payer, and by dollar amount. All three matter, because a code showing up a thousand times might be costing you less than one showing up a hundred times against a single high-value payer. The dollar sort is the one that tells you where to actually focus.
In most practices, three to five lines end up accounting for 65 to 75% of denied dollars. Not sure what’s normal for your specialty? See our average claim denial rates by specialty. Those are the ones you’ll fix over the next 75 days. Everything else, just leave it alone for now.
OmniMD’s medical billing software surfaces your top denial codes with root cause breakdowns by payer, provider, and procedure code, so your team can see exactly which claims are driving the bulk of rejections and close those gaps at the source.
The codes that tend to surface in that top group, for reference:
- CO-16: Claim missing information
- CO-97: Service is bundled
- CO-50: Not deemed medically necessary
- CO-11: Diagnosis inconsistent with procedure
- CO-197: Prior authorization missing
- CO-29: Timely filing exceeded
The discipline these two weeks is just to not start. Don’t fix anything yet, even if you really want to. Practices that skip this and jump straight into fixing what they think the problem is usually end up spending the next 75 days fixing the wrong things. And paying for software they didn’t actually need.
Days 15 to 45: Fix the front end
Once you’ve done the diagnosis, you’ll usually see pretty quickly that most of the problem is at the front desk and intake, not in billing. In most practices, somewhere between 60% and 80% of denials are actually preventable before the claim ever leaves the office. Three changes do most of the work on denial prevention:
Real-time eligibility verification on every patient at every visit. Not just new ones. Coverage changes mid-month all the time, especially for marketplace plans, Medicaid managed care, and employer plans that renew at fiscal year boundaries. A 270/271 check costs you under fifty cents and saves you from a denial that costs 45 days of cash flow plus all the rework.
Prior authorization tracking with one rule: nothing gets scheduled until the auth is confirmed in writing. Not “the rep said it should be fine.” Actual written confirmation, attached to the chart. That one rule by itself reliably kills 15 to 20% of prior authorization denials inside a month.
Custom scrubber edits at your clearinghouse for your top three denial reasons. Say your biggest issue is missing modifier 25 on E&M visits with a same-day procedure. Your medical billing clearinghouse can almost always build an edit that catches that before submission. Compare the top claim scrubbing software options if you’re evaluating tools. Most can do it in an afternoon, and most don’t charge anything extra for it.
Those three changes will stop most of the damage. They won’t fix what your providers are putting in the chart, though, and that’s what the next phase is about.
Days 30 to 60: Show providers their own charts
Generic CPT training doesn’t really do anything. What actually works is pulling denied claims for your top three CPT codes, looking at the charts behind them, and showing providers the pattern. After about ten or so charts, you’ll usually see the same issue popping up. Maybe it’s E&M visits where time isn’t documented but the level was billed based on time. Maybe it’s modifier 25 getting added on every visit with a procedure, whether or not the documentation actually supports a separately identifiable E&M.
Set up a 30-minute meeting. Bring printouts of the providers’ own denied charts, redacted, and just walk through them. Telling Dr. Patel her modifier 25 documentation needs work doesn’t really land. Showing her a chart where she billed 99213 with a 17110, and the documentation reads “lesion noted, treated with cryotherapy” and nothing else, that’s the meeting that changes how she charts the next day.
One thing to set up before the meeting, not after: leadership cover. Otherwise you usually get a lot of nodding and agreement that doesn’t survive the next denial.
Days 45 to 90: Tighten the back end
Even with eligibility, prior auth, and provider documentation in better shape, some denials are still going to come through. Three back-end moves close the loop:
A 48-hour rule on denials. Any denied claim gets worked within two business days. Overturn rates drop fast the longer denials sit, and timely filing windows close quickly (90 days for some payers, 30 for others).
Appeal templates for your top five denial reasons. A good template has the relevant policy language, the documentation supporting payment, and a clear statement of why the denial was wrong. Templates plus chart notes can cut appeal time by more than half, and overturn rates usually go up because templated appeals end up being more thorough than ones written in a hurry.
Tracking overturn rates by payer. If you’re winning 70% or 80% of appeals against one particular payer, that payer is denying claims they shouldn’t be. At that point it isn’t really a billing problem anymore, it’s a contracting problem, and it should be on file for the next time you renegotiate. Most practices skip this entirely, which is part of why most payers just keep doing it.
The habit that holds it all together
Each of the four phases above belongs to a different group of people. The front desk owns intake, providers own documentation, the biller owns appeals. Without something that sits across all three, each phase drifts back to old behavior the moment you stop paying close attention.
Ten minutes every morning is enough. Front desk lead, biller, one provider rep. Just look at yesterday’s denials together. No agenda, no slides.
A normal morning sounds something like this:
- The front desk hears that the auth field they skipped yesterday cost the practice $480.
- The provider hears that two of their charts got denied for missing time statements.
- The biller hears that the new payer everyone keeps complaining about is actually fine, and the established one is denying 12% of claims this month.
Behavior changes faster from this one habit than from any software, training, or policy you’ll ever buy, mostly because each person hears the cost of their own decisions in front of the others.
What ‘good’ looks like at day 90
Track these weekly, not monthly. If any of them starts moving the wrong way, you’ll catch it in seven days instead of seven months.
- Denial rate: under 7% (most practices start somewhere between 12% and 15%)
- Clean claim rate: above 93%
- First-pass resolution rate: above 90%
- Days in AR: under 35
- Appeal overturn rate: above 60%
What 50% in 90 days actually looks like
New practices often hit 60 to 70% reductions because the baseline was so high. Established practices typically hit 50% right at day 90 and need someone with authority to break the existing workarounds. Urgent care hits it through automation more than process. Multi-specialty groups hit it by treating each specialty as its own project.
The practices that miss the goal almost always skipped days 1 to 14 and started fixing before they knew what was broken. Three months later, denials are unchanged and they’ve also paid for software they didn’t need.
If you’re staring at a denial rate you can’t move, start with the data. Or let our medical billing services team run the diagnosis and the fix for you. Find your top five claim denial reasons. Pick the front-end fix that addresses the biggest one first. The rest of your claim denial management work follows from there.
Payers systematically underpay on a share of claims, and most practices never flag it because the claim technically processed. Payer underpayment recovery covers how to identify the gap between contracted rates and actual reimbursement and how to build the appeal workflow that recovers it.

Dr. Giriraj Tosh Purohit is an experienced Product Manager and Security officer with a strong background in healthcare technology and management consulting. With expertise spanning clinical workflows, EHR, RCM, Digital Health, and AI-driven products, he has been instrumental in shaping innovative healthcare solutions.
