
 Written by Dr Girirajtosh Purohit
Written by Dr Girirajtosh Purohit
What Physicians Need to Know About CMS’s 2027 Coding and Documentation Overhaul
What do the CMS coding and documentation changes mean for physicians?
CMS is tightening how diagnoses are documented, coded, and valued in risk adjustment models. This means providers must capture more precise clinical details in their notes to ensure accurate reimbursement. Incomplete or vague documentation may lead to lower risk scores, reduced payments, and increased audit scrutiny. To stay compliant and financially stable, practices must improve documentation accuracy, align coding with clinical evidence, and adopt tools that support real-time, structured charting.
CMS is tightening the rules on how risk gets measured, how diagnoses get valued, and how much scrutiny your documentation will face. Here is what that means for your practice, your patients, and your notes.
If you have been sensing that the documentation pressure in your practice is getting heavier, you are not imagining it. A policy shift is underway at CMS that will directly change how your clinical notes are interpreted, how the diagnoses you record are weighted financially, and how much scrutiny the codes you submit will face. Understanding what is driving that shift, and why it is arriving now, is the starting point for responding to it intelligently.
“The art of medicine consists in amusing the patient while nature cures the disease. But in 2027, the art will also consist in documenting what nature is dealing with, precisely enough to survive a risk model audit.”
Adapted from Voltaire, with a 21st-century addendum
The Policy Signal Behind the 2027 Advance Notice
The CMS 2027 Advance Notic, released January 26, 2026, is more than an actuarial filing. It is a policy declaration. CMS has stated plainly that it believes the 2027 changes will address coding differentials between Medicare Advantage and Original Medicare. That phrase, nested in the opening letter from Center for Medicare director Chris Klomp, is carrying enormous weight.
What CMS is describing is a known, documented, persistent gap between how conditions get coded in Medicare Advantage (MA) versus traditional fee-for-service. As practices transition into value-based care models, understanding this shift is the starting point for responding to it intelligently.
MA plans have historically captured more diagnoses per patient, generating higher risk scores and therefore higher capitation payments. CMS has watched this gap for years.
In 2027, it is doing something about it at the model level, and the effects will flow directly into how physician documentation is interpreted, weighted, and financially valued.
4.04%
Projected MA per capita growth rate for 2027 (aged + disabled)
5.39%
Underlying per capita cost trend driving that growth
6.17%
Per capita growth for ESRD dialysis patients-the most complex tier
That is why this notice matters to clinicians because the decisions being made in this filing will determine what a well-documented note is worth, and what an imprecise one costs.
Why These Changes Land Hard: The Cost Trajectory Behind the Model
To understand why these model changes carry such consequence, it helps to look at where Medicare costs are already headed, because the patients who will be most affected by tighter documentation standards are the same ones whose care is growing most expensive.
Medicare’s sickest patients are getting more expensive to care for, faster than inflation and faster than overall program growth. ESRD patients alone are on a 6.17% per capita annual cost trajectory. These are also the patients whose documentation requires the most precision, and whose care will be most affected by what happens next in the risk model.
In other words, the patients who demand the most clinical attention are also the ones where documentation errors carry the greatest financial consequence. That intersection is where the 2027 changes will hit hardest.
Risk Adjustment: The CMS-HCC model is being retightened. Here is what that demands from your notes.
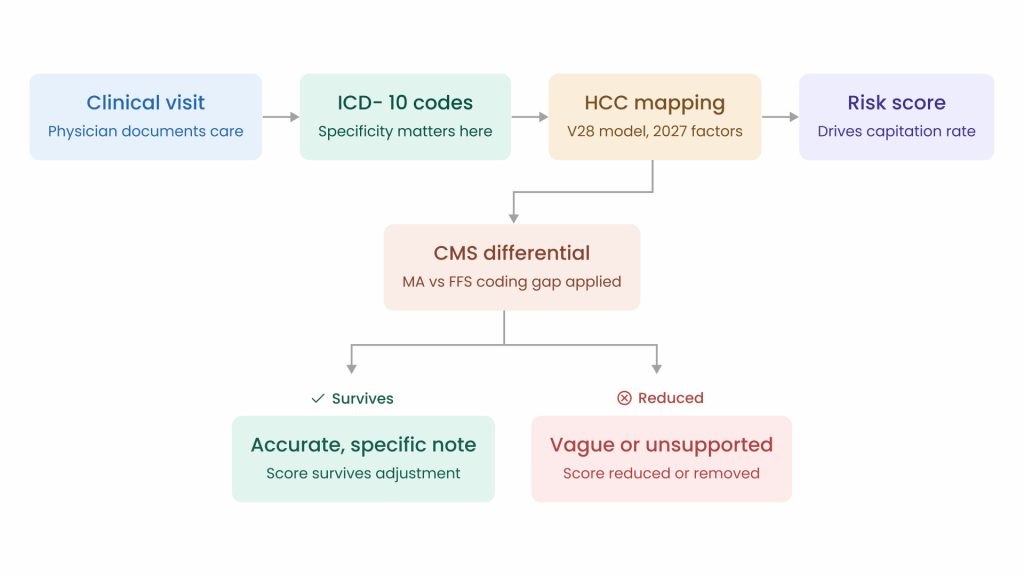
The CMS-HCC risk adjustment model is the engine that converts diagnoses in a patient’s record into a risk score, which in turn determines how much a plan is paid per enrollee. When the model is calibrated generously, imprecise documentation can still produce a usable code. When it is calibrated tightly, only specificity survives. Achieving this level of HCC coding accuracy is what the V28 updates demand from your clinical notes. The 2027 Advance Notice signals a clear move toward the latter.
The notice outlines updates to the V28 version of this model, including revised relative factors across population categories: continuing enrollees, aged and disabled new enrollees, and new enrollees in Chronic Condition Special Needs Plans.
The direction of recalibration matters deeply. The model is being tuned against how patients actually use resources in fee-for-service settings, not against the historically elevated coding patterns observed in MA. That means certain HCCs that have been weighted generously will carry lower relative factors going forward, and conditions that are real but documented imprecisely may not register at all.
“Measure what is measurable, and make measurable what is not so.”
Galileo Galilei- a principle CMS is now applying to diagnosis codes
How Physician Documentation Flows Into Risk-Adjusted Payment
The model is not being redesigned to punish physicians. It is being redesigned to reward accuracy. But that switch puts the burden squarely on the clinical note. Here is what that looks like condition by condition:
- Diabetes: “Diabetes with complications” and “diabetes without complications” map to different HCCs.Following a structured guide for ICD-10 codes for diabetes ensures the difference lives clearly in your documentation.
- Heart failure: Staging, functional class, and etiology all affect how the condition maps. “CHF” alone is not sufficient in a tighter model.
- CKD: Stage matters. Stating the stage once per year, with clinical basis in the note, is what keeps it active in the risk calculation.
- ESRD: With a 6.17% per capita cost growth trajectory, these patients represent the highest documentation stakes in your panel.
- Mental health comorbidities: Often under-documented in primary care despite being active clinical problems that carry real HCC weight.
CMS is filtering its own data for anomalous billing. That should tell you something.
However, the model recalibration is not the only lever CMS is pulling. It is also cleaning up the data it uses to set payment benchmarks, and the way it is doing that sends a clear message about where documentation standards are heading.
One of the less-noticed provisions in the 2027 Advance Notice is a proposed exclusion of significant, anomalous, and highly suspect billing activity in Calendar Years 2023 and 2024 from the ratebook fee-for-service experience.
CMS is building a cleaner dataset by removing billing it considers implausible before using that data to set payment benchmarks.
“In God we trust; all others must bring data. And in 2027, CMS is very specifically deciding which data it trusts.”
W. Edwards Deming, adapted for the modern era of risk adjustment
What this signals for physicians
When a regulatory agency starts explicitly filtering its own datasets for anomalous patterns, it is communicating that it has built the analytical infrastructure to find outliers. The question every physician should be asking is not whether their individual billing is problematic, but whether their documentation would hold up to the kind of scrutiny that is now being applied at the model level. The answer to that question depends entirely on what is in the chart.
What this signals is a change in what “good documentation” means going forward. The old posture was additive, capturing everything that could generate a code. The new posture has to be defensible, every code backed by clinical evidence that would survive scrutiny. Preparing your practice for surviving a medical billing audit is now a core requirement of the 2027 environment.
Physicians who care for the most complex patients, the ones with ESRD, overlapping chronic conditions, active mental health comorbidities, face the steepest documentation requirements at the exact same moment those patients demand the most clinical attention. Which raises the practical question: how are physicians actually supposed to do this?
AI Scribes and the JAMA Study: What the Numbers Really Mean
That question, how to meet a rising documentation standard without sacrificing clinical presence, is exactly what a landmark study published in JAMA in April 2026 was designed to answer.
The study, co-led by researchers from Mass General Brigham and UCSF, covered five academic health systems, tracked over 8,500 ambulatory clinicians for more than two years, and compared 1,809 AI scribe adopters against 6,770 control clinicians at the same institutions.
13 min
Daily reduction in total EHR time per 8 scheduled patient hours
16 min
Daily reduction in documentation time specifically (10% relative decrease)
0.5
Additional patient visits per week among AI scribe adopters
The headline findings, 13 minutes of saved EHR time per day, 16 minutes of documentation time, half a visit per week, have been met with underwhelmed commentary in some corners of medicine. That reaction is understandable, but it misses where the real value is.
“We do not rise to the level of our expectations. We fall to the level of our tools. The question for 2027 is which tools physicians choose to fall back on.“
Archilochus, interpreted for the documentation era
The more important finding is what happened among clinicians who used AI scribes for 50% or more of their visits.
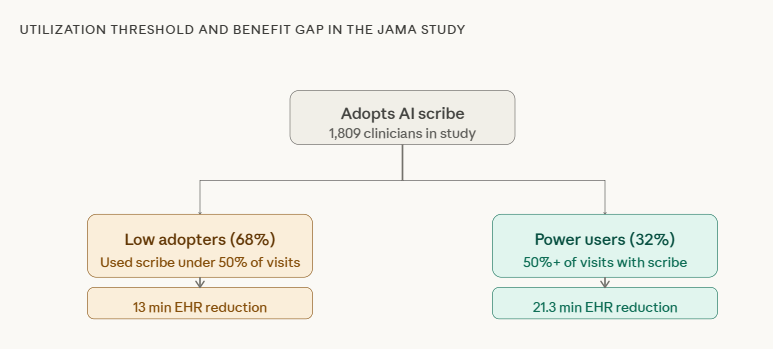
Power users, those who applied the tool consistently, experienced over twice the reduction in total EHR time and three times the reduction in documentation time. The technology has a utilization ceiling problem, not a capability problem. Implementing a purpose-built AI medical scribe for clinicians is the most direct way to cross the threshold where benefits become meaningfully larger. Only 32% of adopters crossed the threshold where the benefits became meaningfully larger.
WHO BENEFITED MOST
The most pronounced improvements were observed among primary care physicians, advanced practice providers, and female clinicians. Primary care is precisely where the HCC documentation burden concentrates, because that is where chronic condition capture happens annually, where the diagnoses that feed the risk model get refreshed, and where the coding differential CMS is trying to close has historically been most significant.
Why the $167 Monthly Revenue Figure Is the Wrong Number to Lead With
Media coverage of the JAMA study led with the $167 monthly revenue finding, which frames the value of AI scribes entirely through a throughput lens. But in a 2027 payment environment, throughput is not the point.
THROUGHPUT FRAMING (WRONG LENS)
- Can I see 0.5 more patients per week?
- Will I earn $167 more per month?
- Is the ROI positive on the subscription cost?
DOCUMENTATION QUALITY FRAMING (RIGHT LENS)
- Are my chronic condition diagnoses captured annually with specificity?
- Is the clinical basis for each HCC-relevant code present in the note?
- Would my documentation survive the scrutiny CMS is now building into its models?
The freed cognitive bandwidth during a visit is not best measured in additional appointments scheduled. It is best measured in whether a physician, no longer mentally composing a note while examining a patient, captures the nuanced clinical picture that the 2027 HCC model will require.
The study authors noted that clinicians may be reallocating their recovered time into reviewing prior documentation, responding to patient messages, and spending more face-to-face time in the room. Each of those activities directly feeds the quality of the clinical record, which is exactly what the 2027 model is designed to reward.
“The doctor of the future will give no medicine but will interest his patients in the care of the human frame, in diet, and in the cause and prevention of disease.”
Thomas Edison-who also understood that the right tool changes what is possible
What this means by role
The 2027 changes do not land the same way for every clinician. Here is where the stakes are sharpest by role:
- Primary care physicians: The annual chronic condition documentation that feeds HCC scoring happens in your office. Using specialized primary care EHR software ensures that precision becomes a natural part of your workflow. The 2027 model updates make precision there more consequential than ever.
- Specialists: Conditions you document, even in consultation notes, can contribute to a patient’s MA risk score. Specificity in your notes matters across the care continuum.
- Advanced practice providers: The JAMA study found APPs among those who benefited most from AI scribe adoption. The documentation burden on APPs in primary care is proportionally higher — and so is the upside of addressing it.
- Medical directors and CMOs: The 2027 changes create a practice-level incentive to invest in documentation infrastructure now, before the rate announcement finalizes in April 2026.
The Bottom Line: CMS Wants the Model to Be Honest. The Burden of That Honesty Falls on the Chart.
CMS’s goal is not to make medicine harder. It is to make the payment model reflect clinical reality more accurately. That is a defensible objective. But the practical effect of pursuing it through model recalibration, differential adjustments, and anomalous billing exclusions is that the documentation bar rises most steeply for the physicians who care for the most complex patients.
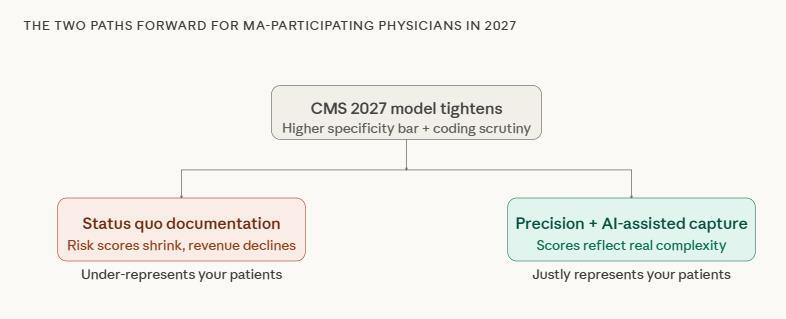
Those two pressures, document more precisely, while caring for patients who demand more of your attention, do not have to be in conflict. But resolving them requires more than a coding strategy or a compliance checklist.
If the 2027 overhaul pressures physicians to document more precisely while they are already stretched thin, and if AI scribes offer a real, evidenced, but underutilized path toward recovering some of that cognitive capacity, then the most consequential decision many physicians can make in the next twelve months is not about coding. It is about whether they are willing to actually adopt an AI medical coding solution that could make the precision CMS is demanding feel less like a regulatory burden.
CMS is asking for documentation that reflects clinical truth. The JAMA study is showing that there are tools available to help physicians deliver it without burning out. The gap between those two facts is not regulatory. It is a utilization gap, a behavioral gap, a decision that will be made practice by practice, physician by physician, in the months before the 2027 rate announcement finalizes. The physicians who close that gap first will not just be better positioned for 2027. They will be better physicians for their most vulnerable patients, which was the point all along.

Fix Documentation Gaps
Avoid revenue loss from incomplete clinical notes.